I saw Mr SM 36yo new patient for sequential altitudinal vision loss at 20yo and then 36yo. Was wondering if you would label him as optic neuritis and put him on long term immunosuppression .
Background: nil
Ocular: nil
Fhx: nil fhx migraines. Father Addison's disease. Brother haemolytic uremic syndrome. Mother parkinsons. Nil vision loss.
Medications: nil.
Social: occupational health. Home with partner and 2 kids. Nil smoker. Occasional alcohol
2009 Age Was working at Crown Casino and had blurring os and thought he had a hair in the way os. 2 days later went to GP and still had the stripe os. 5 days from Crown woke up with inferior vision loss od. Had mild tension around the eyes and uncomfortable to move eyes in extremes. Then went to a GP and then Hospital 23Oct2026. Maintained visual acuity of 6/5 od and os. Notes reports inferior field defect od superotemporal quadrant loss os. ophthalmology notes bilateral disc swelling ou . He was diagnosed with bilateral optic neuritis. His vision loss never progressed and never improved with IVMP steroids. MRI brain 26Oct09 and whole cord 19Nov09 normal. NMO -ve. Had repeat MRI brain and spines in 2010, 2011, 2012 and then 2013. No change and never any lesions to suggest chronic ischaemic change or demyelination.
Had persistent inferior field defect od and stripe of vision os since the initial onset.
Seen in 2016 and NMO and MOG -ve
26Dec25 was walking down stairs in Queensland and noticed had a cloud inferiorly os and uncomfortable to move the eyes. Went to Sunshine hospital had IVMP and had a lumbar puncture. Glucose 4.2 Protein 380 (150-500) wbc 1 rbc 2 culture negative.
Lupus -ve, folate 46.5 b12 474, syphilis -ve, quantiferon -ve, strongyloides -ve, HIV -ve, HTLV -ve, CMV -ve EBV IgM and VZV IgM-ve, RF <20 anti ds DNA -ve ANCA -ve, ANA -ve. SPEP -ve. Had disc swelling os. Went on prednisolone for 3 weeks post. Swelling started to reduce after a week.
NMO -ve MOG -ve CSF MOG -ve
OPSM
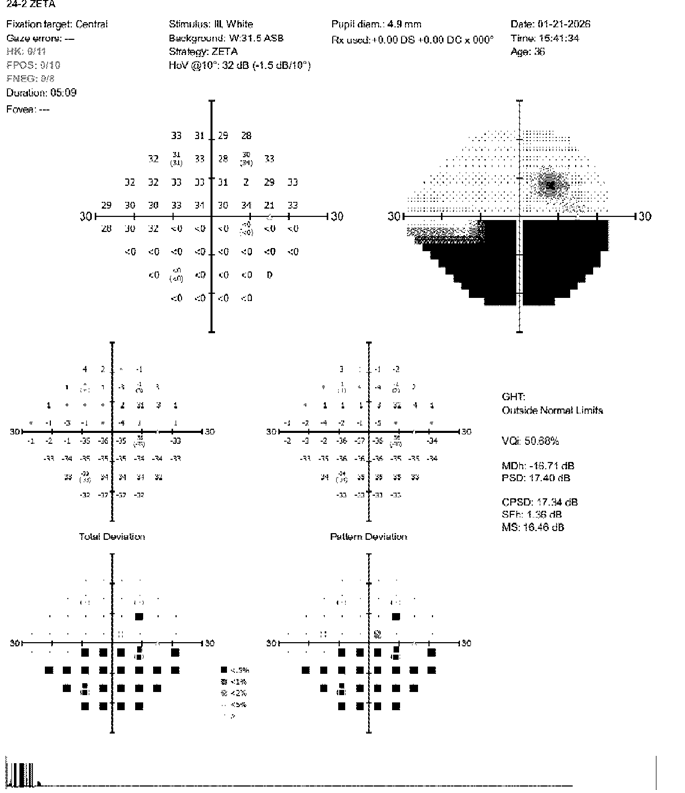
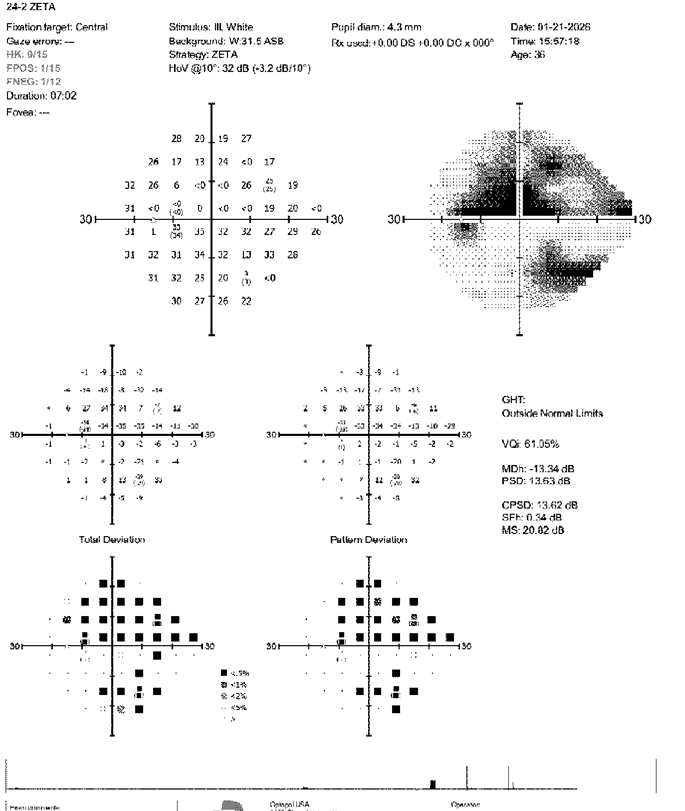
21Jan26 HVF inferior field defect od superior arcuate with an island inferonasally loss os
21Jan26 OCT RNFL 68um od 97um os
Started mycophenolate 2g daily. He took it for 3 weeks and stopped because of flu like symptoms and found it inconvenient to take medication. You organised CT Chest and this showed no sarcoidosis. Completed on 8Apr2026.
Apr2026 was reading a computer screen and had depth perception loss, letters missing, swirly lines. Could see with eyes close. Didn't evolve. Was in both eyes. Went to lie down for 15-20 minutes and was sensitive to light and then got frontal headache. No residual loss. Took Panadol.
3 days ago, similar episode. Both episodes were post gym work out. 1-2 hours post workout.
No day time napping. Snores only if on his back.
Exam: BP 119/72 HR 62
VA 6/5sc od 6/5sc os CP 7/7 ou, confrontational visual fields inferior field defect od – cannot detect movement inferiorly od, blurring inferiorly os – counts fingers normally. Describes stripe of vision loss superiorly os
Pupils 3mm ou in light 5mm ou in dark. No RAPD. Fundoscopy: pale disc od inferior pale os – disc at risk os.
Full eye movements
Investigations:
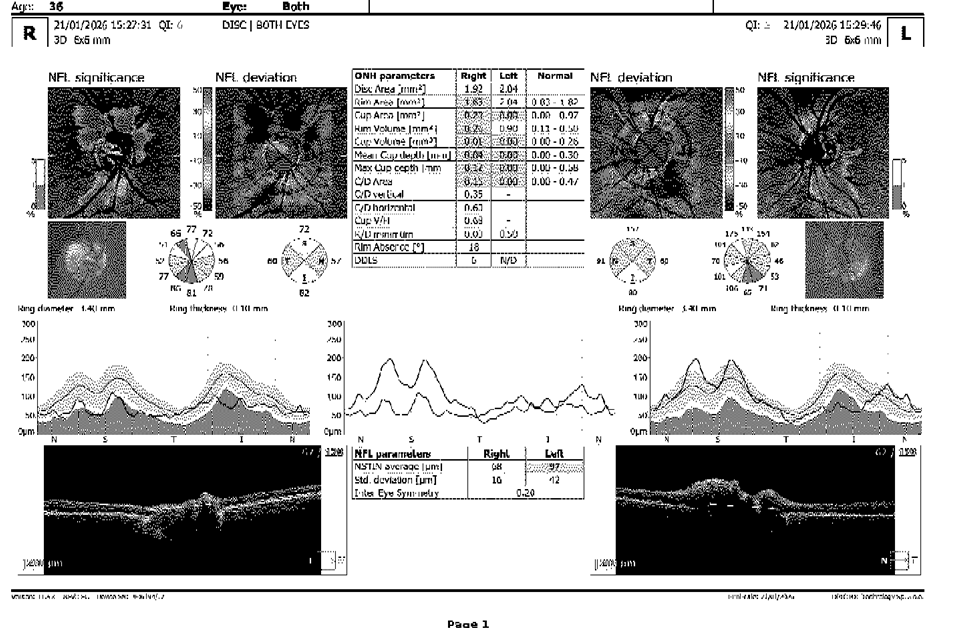
Sorry I dont have any OCTs in colour. I happened to see him in a room that doesnt have this equipment
Impression: 2009 describes sequential sudden onset altitudinal vision loss os then od with no progression and no improvement with steroids. 2025 again sudden onset altitudinal vision loss os with no progression and no improvement of steroids. Given he has disc at risk I cannot go past NAAION as a diagnosis. This is altitudinal, sudden onset, typically painless – but can have pain in 10-15% and doesn't respond to steroids.
Plan: fasting cholesterol, TAG, HDL, LDL, fasting glucose.
Will discuss with my colleagues about him.