Yes, I agree that the discs don't look all that impressive in the optos photos, but there is a clear asymmetry clinically, with the right disc being more elevated and hyperemic compared to the left. I thought the 10um difference and superior thickening on OCT confirmed my clinical impression.
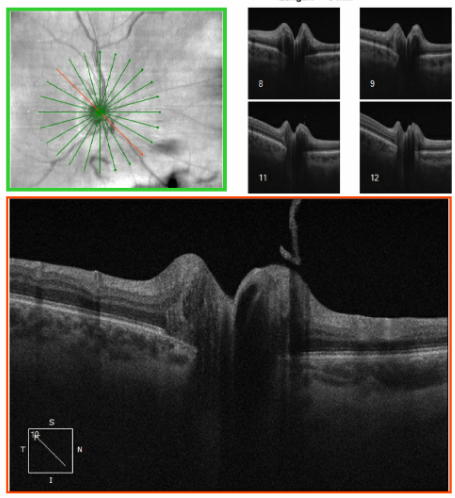
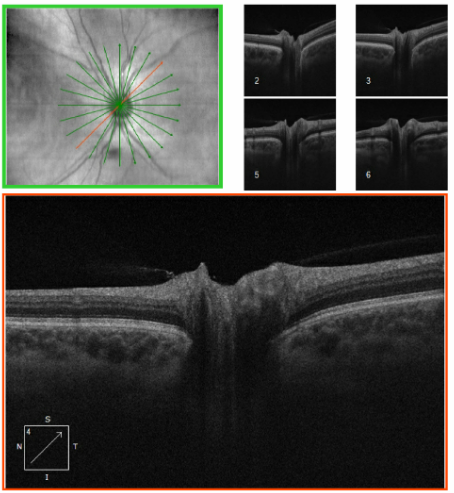
As for EDI OCT, our Heidelberg is currently down, so I got the deepest images I could on the Cirrus, but I feel confident about the lack of ODD (our study with Steffen showed that FAF is still pretty darn good). I did try to capture the one slice that showed the little papillary tuft, although I'm not convinced that it's enough (or in the right location) to be the cause.
For the surgical approach, a buckle without vitrectomy is the plan, since she is so young and so myopic. If she gets a post-vitrectomy cataract in that eye, she will not be able to tolerate the anisometropia if we fix it, which opens up a whole new set of issues.
I think/hope I've answered all the questions.. As always, I appreciate everyone's input!
Lulu
The information transmitted is intended only for the person or entity to which it is addressed and may contain confidential and/or privileged material. Any review, retransmission, dissemination or other use of, or taking of any action in reliance upon, this information by persons or entities other than the intended recipient is prohibited. If you received this in error, please contact the sender and delete the material from any computer.
www.sjhc.london.on.ca
Original Message:
Sent: 7/10/2025 7:16:00 PM
From: Eric Singman
Subject: RE: Retinal detachment and optic disc edema
Where do we stand on PVD and NAION? Possible "mild" case. VEP?
Original Message:
Sent: 7/10/2025 6:38:00 PM
From: Christine Greer
Subject: RE: Retinal detachment and optic disc edema
Hi!
I bet a PVD caused both a tear & detachment and also caused some traction at the disc as the vit separated off the optic nerve head. Is these a Weiss ring? I’ve seen real time disc edema and hemorrhage occur during RD repair when the surgeon is inducing a PVD. It’s wild.
Wouldn’t stop the surgeon from doing a buckle if that’s what’s indicated from a retinal perspective.
Christine
Original Message:
Sent: 7/10/2025 5:22:00 PM
From: Matthew Kay
Subject: RE: Retinal detachment and optic disc edema
If these are the photos of the patient that was described as having optic nerve edema with a retinal detachment, these optic nerves do not appear to be swollen in the least.
I would do absolutely nothing from a neuro-ophth perspective.
Matt
Sent via the Samsung Galaxy S21 5G, an AT&T 5G smartphone
Original Message:
Sent: 7/10/2025 1:41:00 PM
From: Lulu Bursztyn
Subject: RE: Retinal detachment and optic disc edema
Thanks everyone for your input, and an interesting debate on Occam's razor...
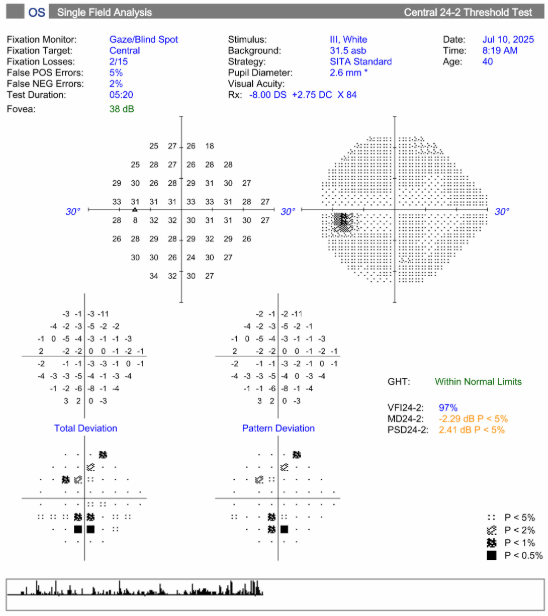
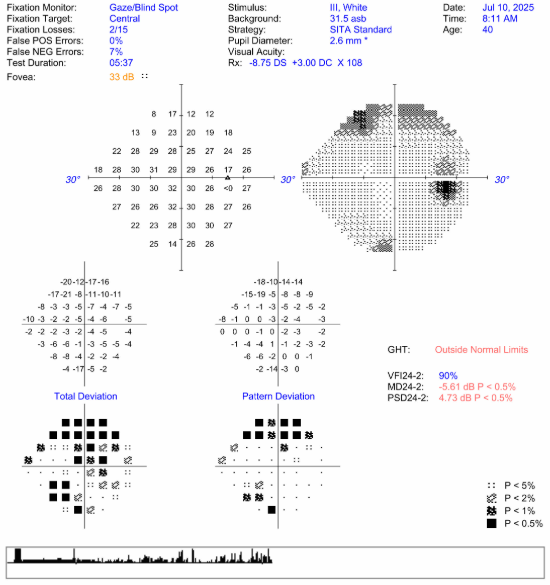
Some updates, now that I've had a better look at her, and hopefully the images come through. She describes new floaters starting one week ago followed by a superior curtain defect over the past few days. Prior to this vision was her normal. Visual acuity remains 20/80 R, 20/20 left, colour 16/16 OU. IOP was 15 OU this morning. I actually cannot detect an RAPD despite the complaint of subjective decreased brightness. Anterior chamber is quiet, no vitritis, just a lot of vitreous syneresis (this is what I mean by turbid – very thick strands of floaters). There is an inferior temporal hole in the RD. There is bilateral fairly symmetric inferior RNFL thinning that I suspect is related to her high myopia, but there is also superonasal edema of the right disc. The visual fields show a superior field defect in the right as well as a small inferior defect in both eyes. I have requested an MRI (this is Canada, it's not happening today...) and have sent her for some blood work (CBC, CRP, syphilis, ENA, mitochondrial panel...). I will also see her back after the RD is fixed.
Lulu

Hole visible inferotemporal
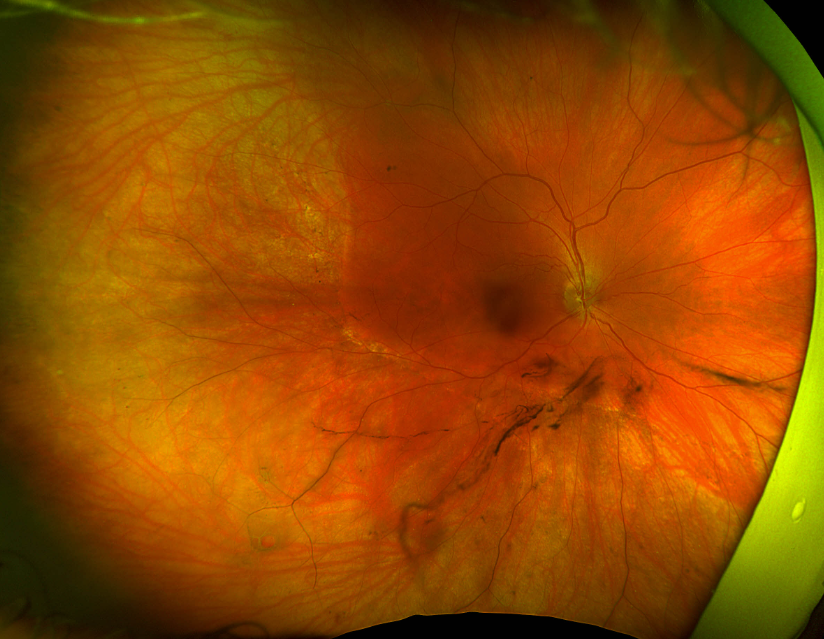
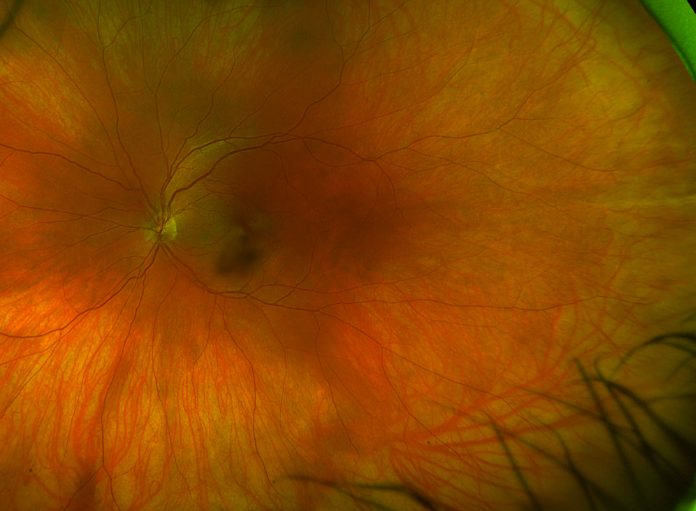
FAF, no visible ODD, but the RD really stands out nicely

Lulu Bursztyn
Comprehensive and neuro-ophthalmology
Western University, London, Ontario
lulu.bursztyn@sjhc.london.on.ca
519-646-6214
The information transmitted is intended only for the person or entity to which it is addressed and may contain confidential and/or privileged material. Any review, retransmission, dissemination or other use of, or taking of any action in reliance upon, this information by persons or entities other than the intended recipient is prohibited. If you received this in error, please contact the sender and delete the material from any computer.
www.sjhc.london.on.ca
Original Message:
Sent: 7/10/2025 11:27:00 AM
From: Sherif Ahmed Kamel Abdelbar
Subject: RE: Retinal detachment and optic disc edema
Things are not so simple especially when it comes to neuro-ophthalmology or retinal problems , then combined proposed simplicity may be a walking door to problems
Original Message:
Sent: 7/10/2025 11:14:00 AM
From: Scott Forman
Subject: RE: Retinal detachment and optic disc edema
I think Occam's razor is an outdated concept developed before medicine got as complex as it is. Multiple problems (not necessarily totally unrelated) are common and yes they occur in the same body but many are handled by different approaches.
+=+=+=+=+=+=+=+=+=+=+=+=+=+=+=+=+=+=+=+=
Scott Forman, MD
Senior Fellow North American Neuro-ophthalmology Society
Adult and Pediatric Neuro-ophthalmology
Comprehensive Ophthalmology
Functional Medicine
Original Message:
Sent: 7/10/2025 10:42:00 AM
From: Joseph Chacko
Subject: RE: Retinal detachment and optic disc edema
Your "plan is to treat it like 2 unrelated problems."
I would disagree, I'm going with Occam's razor on this one. Let the retina specialist fix the RD, and then monitor the disc edema, it should resolve.
Confidentiality Notice: This e-mail message, including any attachments, is for the sole use of the intended recipient(s) and may contain confidential and privileged information. Any unauthorized review, use, disclosure or distribution is prohibited. If you are not the intended recipient, please contact the sender by reply e-mail and destroy all copies of the original message.
Original Message:
Sent: 7/9/2025 9:56:00 PM
From: Lulu Bursztyn
Subject: RE: Retinal detachment and optic disc edema
IOP was 12 in the affected eye, 15 in the other. So a little low, but not that asymmetric. No uveitis, although the vitreous was a little turbid. It's a big RD (about 1/3 of the retina), so I agree, there could be an RAPD from the RD and not the nerve. No shifting fluid, and nothing that would make me think VKH. I'm hoping an HVF will help, but my plan is to treat it like 2 unrelated problems.
If it was something compressive, like an ONSM, does anyone think there's a risk putting on a buckle?
The information transmitted is intended only for the person or entity to which it is addressed and may contain confidential and/or privileged material. Any review, retransmission, dissemination or other use of, or taking of any action in reliance upon, this information by persons or entities other than the intended recipient is prohibited. If you received this in error, please contact the sender and delete the material from any computer.
www.sjhc.london.on.ca
Original Message:
Sent: 7/9/2025 7:56:00 PM
From: Andrew Carey
Subject: RE: Retinal detachment and optic disc edema
Some myopes will have peripapillary schisis that looks like disc edema, you can tell the difference if you look closely at the cross sectional OCT over the optic disc. Myopes are also common to have pseudopapilledema from tilted discs.
At Iowa, they found that for each quadrant involved by RD you get a 0.3 log unit RAPD. So, a mild RAPD may be retinal rather than indicating optic neuropathy in your case.
Did the retina doctor identify a break that is causing the RD? Is the fluid gravity dependent/ shifting to suggest it is exudative rather than rhegmatogenous? There are conditions that can cause exudative RD and disc edema (VKH and posterior scleritis are the most common).
Uveitis with retinitis (particularly infectious causes such as toxoplasmosis and viral etiologies) can cause papillitis as well as retinal breaks leading to RD.
A wife field fluorescein angiogram might be helpful.
Best,
Drew
Original Message:
Sent: 7/9/2025 7:30:00 PM
From: Russell Edwards
Subject: RE: Retinal detachment and optic disc edema
Ocular hypotony, vitreo-papulary traction?
Original Message:
Sent: 7/9/2025 7:26:00 PM
From: Jeffrey Odel
Subject: RE: Retinal detachment and optic disc edema
What was tension? Sometimes RDs can have hypotony which may lead to disc edema?
Original Message:
Sent: 7/9/2025 7:11:00 PM
From: Lulu Bursztyn
Subject: Retinal detachment and optic disc edema
Dear all,
I was just asked today by my retina colleague to see a patient with optic disc edema. She is a 40 year old high myope (-10 OU) who noted a blurred vision and floaters in the right eye 2 weeks ago. She was found to have an inferior retinal detachment and referred to retina, who saw her today and noted disc edema in the same eye. She felt that the RD looked older than 2 weeks as there is a prominent demarcation line. Vision is 20/70 in that eye (previously known to be 20/20), but the RD is only up to the inferior arcade, and the amount of vitreous debris does not seem like enough to cause that big of a reduction. OCT macula is normal with no subretinal fluid. I had a quick look today, but she was already dilated. She describes subjective decreased brightness in that eye, and Ishihara colour plates were full, but slower compared to the other eye. Disc edema is grade 2, more prominent inferior than superior, no hgb, and no ODD on EDI OCT or FAF. The plan is to do a scleral buckle on Monday without vitrectomy. I'm bringing her back tomorrow morning to do a visual field and check pupils, but I have 2 questions:
-
Is there a way to connect the optic disc edema with the chronic appearing RD? Or is this most likely 2 separate processes?
-
Is there any reason to avoid a buckle in this setting?
Thanks for your wise words!
Lulu
The information transmitted is intended only for the person or entity to which it is addressed and may contain confidential and/or privileged material. Any review, retransmission, dissemination or other use of, or taking of any action in reliance upon, this information by persons or entities other than the intended recipient is prohibited. If you received this in error, please contact the sender and delete the material from any computer.
www.sjhc.london.on.ca