44yo woman with bilateral recurrent branch retinal arteriolar occlusions associated with headache/migraine. ? Ocular Susacs. ? Recurrent retinal migraine with infarction ?cerebroretinal angiopathy. ?TREX1
Background: migraines started in 30s post delivery of second child. 3-4 migraines per year and had vertigo associated with it.
Ocular nil
Fhx: Father: Bowel cancer. Heavy alcohol use. Peripheral vascular disease with lower limb stents. Mother: healthy. 1 brother and 2 sisters – well. Maternal grandmother – dementia in late 80s. Maternal grandfather had ? MS. Wheel chair. Dx in 20-30s.
Medications: aspirin 100mg daily, endep 20mg nocte
Social: School teacher. Non smoker, nil alcohol. G5 P3 – miscarriage under 9 weeks.
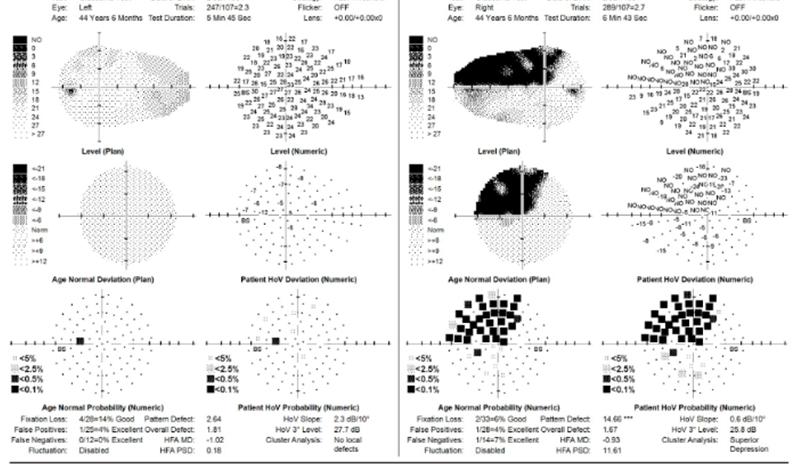
Sep2024 inferonasal blur in right eye then headache following. HVF – inferonasal defect and superonasal defect (patient unaware of) od and normal os. CRP <1 ESR 6
Right superotemporal branch retinal arteriolar occlusion. Started on aspirin 100mg daily and endep. 10mg nocte. ECG sinus. Transthoracic echo normal.
24Jul2025 Carotid US -normal
CT brain and COW 23Jul2025: normal
CT C A Pelvis – normal
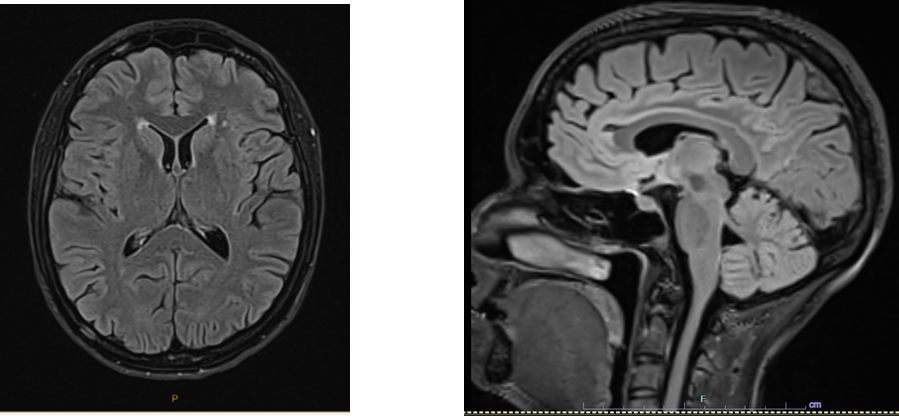
MRI brain: mild chronic ischaemic changes.
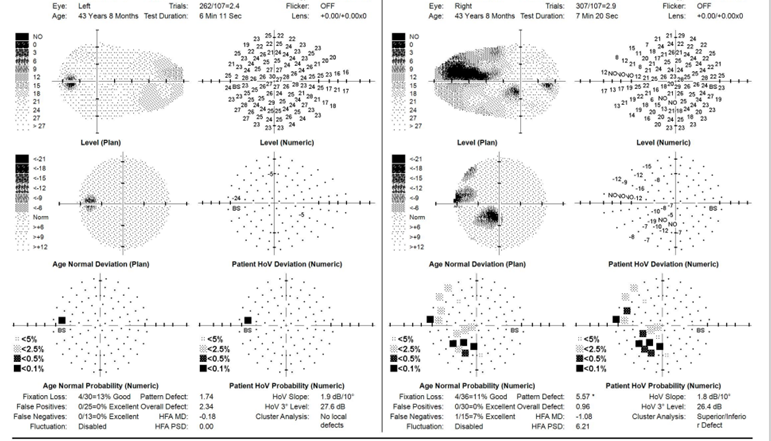
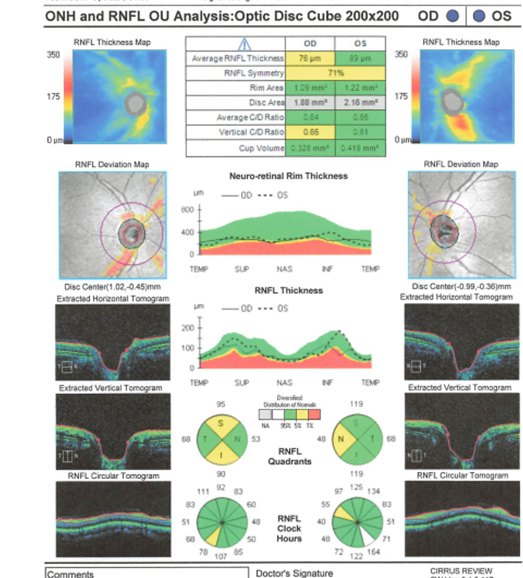
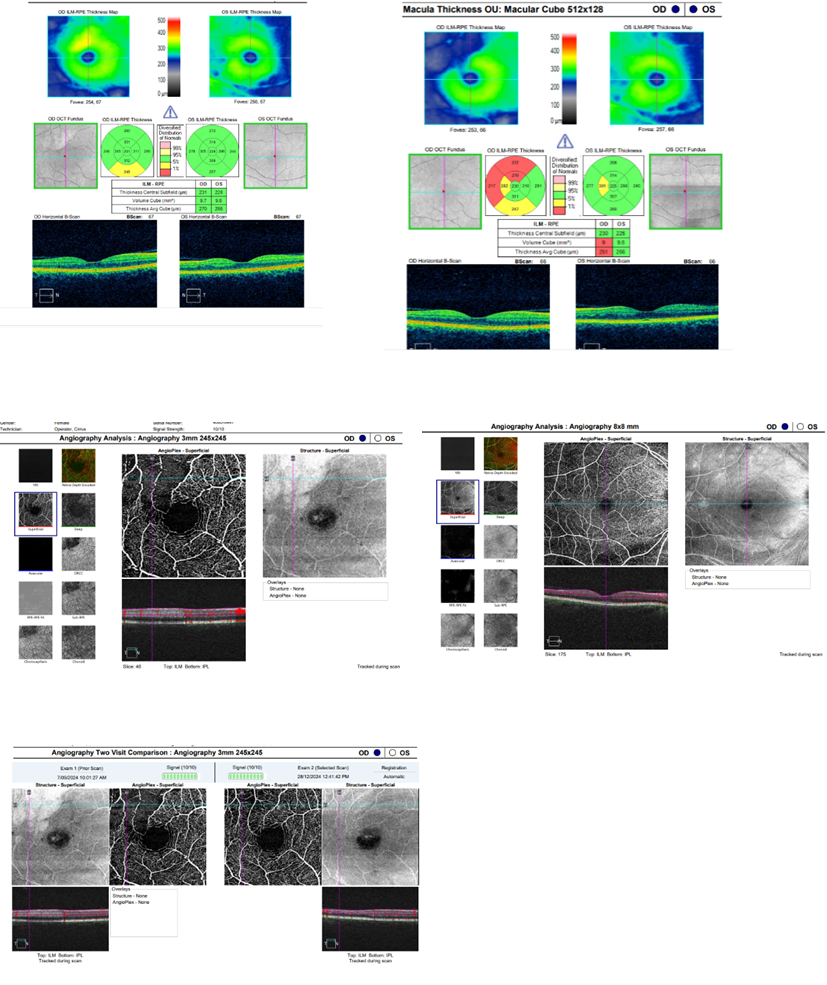
With evidence of old occlusive disease in both eyes as evidenced by inner retinal loss on OCT. The right eye occlusions were larger and had associated field loss.
June2025 headache and seeing floater right eye
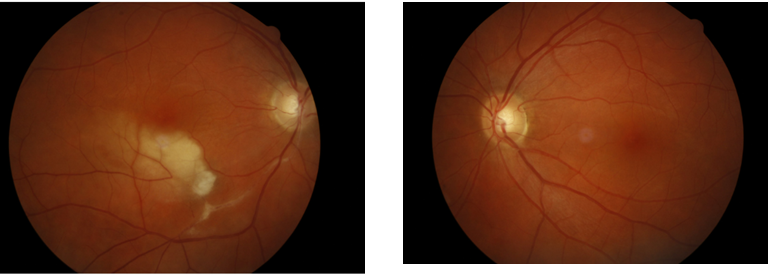
Cotton wool spot inferior to optic disc od. associated with Headache. Endep increased to 20mg nocte
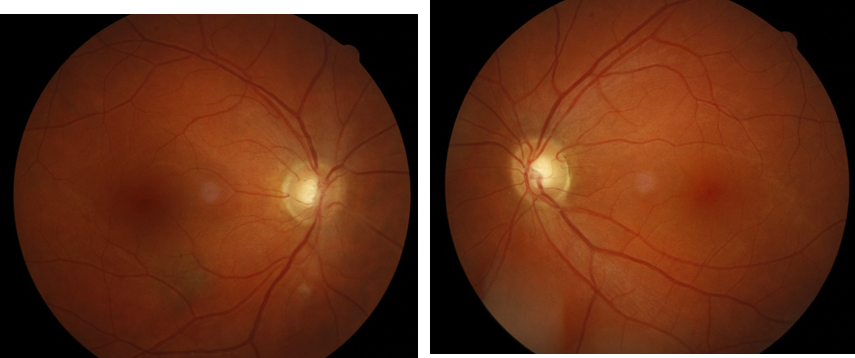
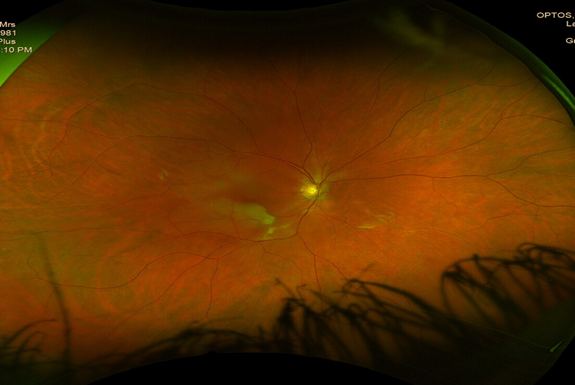
Jul2025 – lost top half of vision superonasally od – completely black out superiorly and then headache started when the vision loss occurred. Optos – BRAO infero pale retina with periarterioloar sheathing. No CWS/ No emboli OD normal OS.
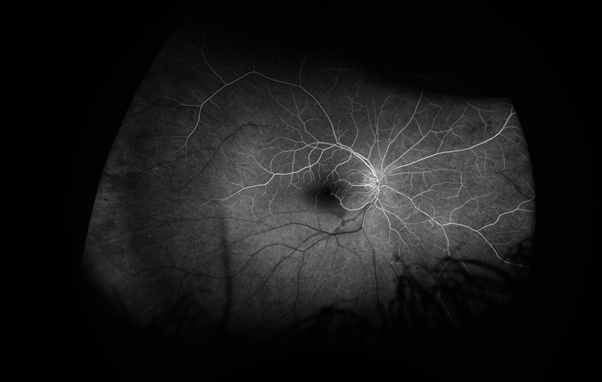
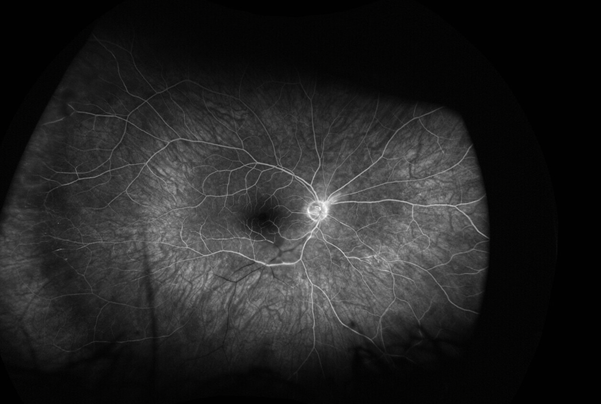
Angio shows complete occlusion inferior temp branch retinal artery. IN early shot can see that there is delayed filling of the superior temp artery (consistent with previous occlusion in Sep 2024).
Left eye only have late shots.
Picture 1. RE – early (30s)
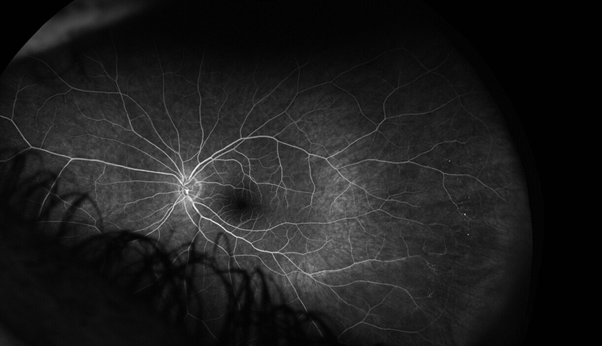
Picture 2 .RE – late (>4 mins)
Picture 3. LE – late (> 4 mins)
RE 23/7/25 retinal oedema along inferior hemi artery with sheathed inferior temp branch > inferior nasal
No history of hearing loss and no episodes of confusion.
Exam: VA 6/6 sc ou CP 7/7 ou, visual fields as documented. No RAPD. Fundoscopy as above.
Full eye movements, nil facial weakness, numbness. Normal tongue movements. Upper limb – nil upper limb drift, normal reflexes and sensation. LL: normal gait and tandem gait. Reflexes intact with downgoing plantars. Sensory examination normal.
7Sep24 Antithrombin III 100% (80-120), protein C 108% (70-150), protein C free 85% Lupus anticoagulant negative, cardiolipin 3 (<10) HbA1c% 4.7% homocysteine 9.7 (4.4-13.6)
Beta 2 glucoprotein 3 (<7)
APC resistance normal. Prothrombin mutation negative.
ANA <160, ANCA -ve, syphilis -ve, HIV -ve. Hepatitis B and C serology -ve, quantiferon -ve. SPEP normal, ACE 32. Lipids chol 4.6 LDL 2.2 HDL 2.0 CRP <5
JAK2 negative, antiphospholipid ab -ve, carotid US normal.
Repeat. CT brain and MRI brain MRA normal. Mild chronic ischaemic change.
ECG sinus. TTE with bubble study – negative for PFO. Heart bug 30 day holter
OCT A – reduced perfusion superotemporally od and normal os. Holter normal ECHO normal. Heart bug – 30 day holter – normal
Retinal colleague states unusual retinal infarcts seen on the FA -delayed filling od both superior and inferior retinal arteries – however they did completely fill. No evidence of vasculitis and no disc leakage.
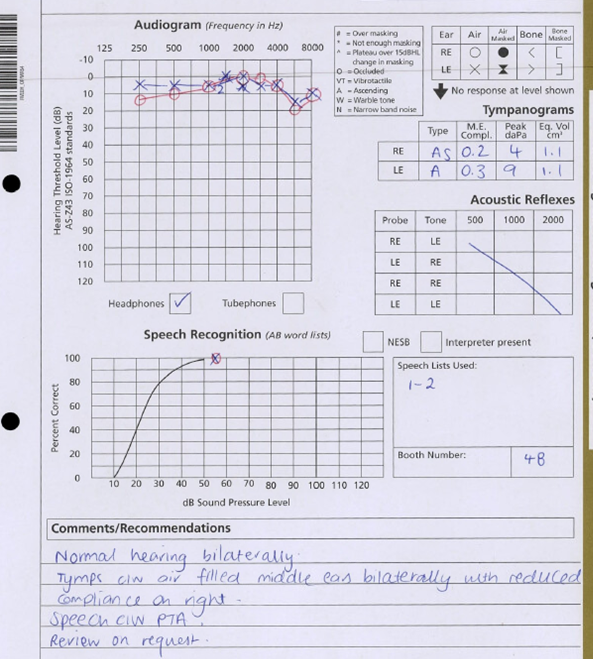
Audiometry normal
Awaiting TOE and ?loop recorder
MRI – no T2 callosal lesions – chronic ischemic change
Regards
Dr Anthony Fok
Neurologist/Neuro-ophthalmologist
Royal Victorian Eye and Ear Hospital/ Monash Health/Melbourne Health